After years of keeping my calendar 📆 on my phone, I’ve gone back to using a paper planner and notebook. The folks at Elmwood Stationers in Berkeley helped me to rediscover the Quo Vadis Trinote Planner. My brain 🧠 likes it already. For example, I need fewer calendar “reminders” or alerts.
It’s good to reconnect with acoustic version of myself. James Wogan unplugged, an analog man in a digital world 💫💛🌎
P.S. – If you’re a young person who’s never used a paper planner, r u abouta check it out?
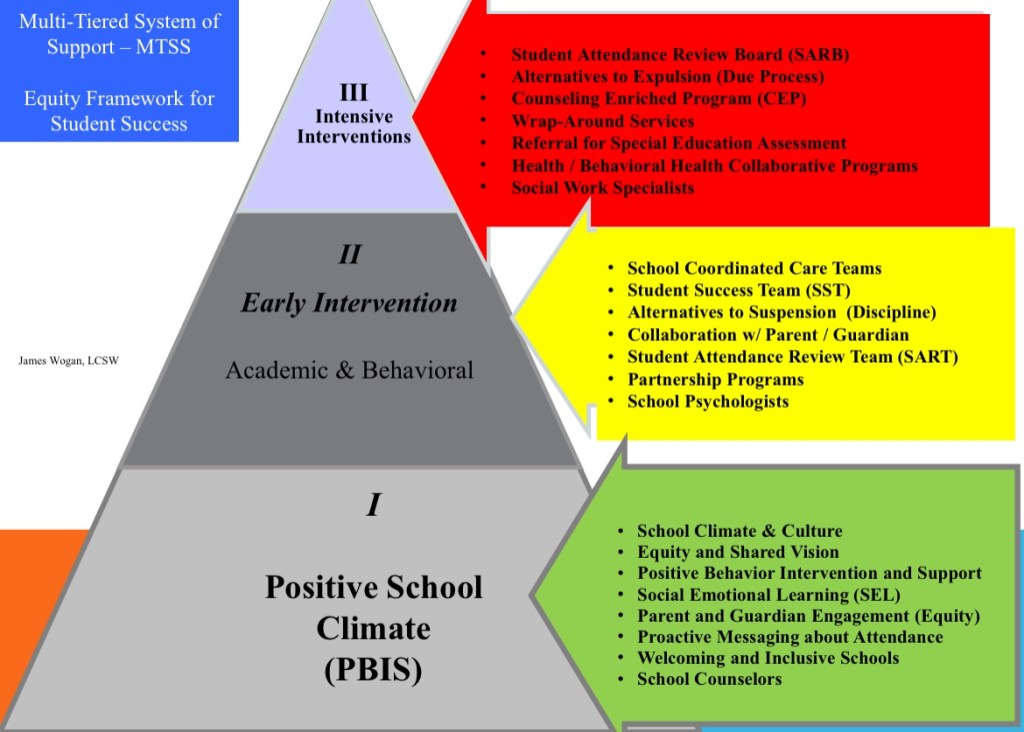
I recently consulted with an agency about School Coordinated Care Teams and the over identification of African-American children in Special Education, known as “Significant Disproportionality.” Utilizing ‘Expanded Equity Partnerships,’ school-based support services are managed and coordinated by School Coordinated Care Teams.
Leaders in this District insist that School Coordinated Care Teams are “MTSS Tier 1.” For example, District says “There’s no point is doing Tier 2 and Tier 3 interventions if schools aren’t doing Tier 1 (PBIS School / Climate) with fidelity.” This misunderstanding is widely held, but only partially accurate. School climate is very important to be sure, but usually not the source of trauma, hardships, and stressors many students face.
Unfortunately, support services are currently stalled out for many under-served students. MTSS was not developed to deny support services to children, but sometimes, this is what plays out.
A rising tide does not lift all boats equally.
Fortunately, we have more opportunities to support kids. Let’s work together on systemic social justice issues, access to behavioral health services, and access to education, i.e. all three tiers concurrently.
I recommended books, Developing your School’s Student Support Teams, Street Data, excellent work of Zaretta Hammond, and publications by West Ed, Break Barriers, and others.
We ask teens, “What % of your life (what you think, how you feel, things you do) do your parents know about?” Average answer: 15-20%. Wait what? Yuhuuup.
Teenager: “My father didn’t know about my ‘secret sugar’ ‘n all but yk, now I’m kiiiinda glad he does”.
The process of immigrating to a new country and acclimating to a new culture can be simultaneously challenging and rewarding. Leaving family, friends, and familiar surroundings creates uncertainty and anxiety for many recent immigrant and refugee families. At the same time, friendships and positive relationships established soon after arriving in a new county often last a lifetime.
Even immigrants with extensive professional experience in their countries of origin may need assistance to navigate public education and local resources. Many recent immigrant families report they appreciate guidance and support while they’re assimilating to the U.S. Schools and community agencies can be valuable partners as families maintain and uplift their culture and heritage. Celebrate diversity and prepare to learn a lot from people who recently emigrated to the U.S.
I try to avoid the term “newcomer” because it belies the hardships and trauma many students and families have experienced. The term “refugee” in this layperson’s post, means people who fled or were evacuated from their previous country in order to avoid harm, persecution and death.
Not all recent immigrants are legally homeless, however, School Social Workers and others collaborate and offer assistance for recent immigrants families. We serve families who are vulnerable oppressed and living in poverty, regardless of immigration status. (See NASW code of ethics).
It’s the expectation that recent immigrant students will show evidence of the immunizations required to attend school. To support immediate enrollment, school district and child-serving agencies link families with resources with information so they can obtain primary care and immunizations asap.
Contra Costa County Public Health offers free immunizations, for example at the Clinic on Stanwell Circle.
This information is shared with parents and guardians by HOPE, CWA’s, Nurses, and school staff members.
Please note: Homeless report forms are not “applications.” Homeless students are identified by site personnel each school year.
Not all recent immigrants are legally homeless. A student living with a family member in a stable home environment, for example, is not automatically considered homeless. If you have questions, every school district has a Homeless Education Liaison. In addition, County Offices of Education offer support and assistance enrolling and supporting students in school.
“Making a big school districts feel small;” Connect and form partnerships with refugee-serving agencies; this helps families to have a better understanding of how to navigate health care, public education and mental health resources in the U.S. Children are assigned grade level based on age, not language, previous school experience, or current learning levels. Adult Education and Early Childhood programs and classes are offered by region, i.e. persons do not need to meet residency requirements to participate.
For further information and up-to-date guidance, see information and “Dear Colleague” letters from US Dept. of Education, California Department Education, and CDSS
Our shared vision is students smiling and doing well in school.
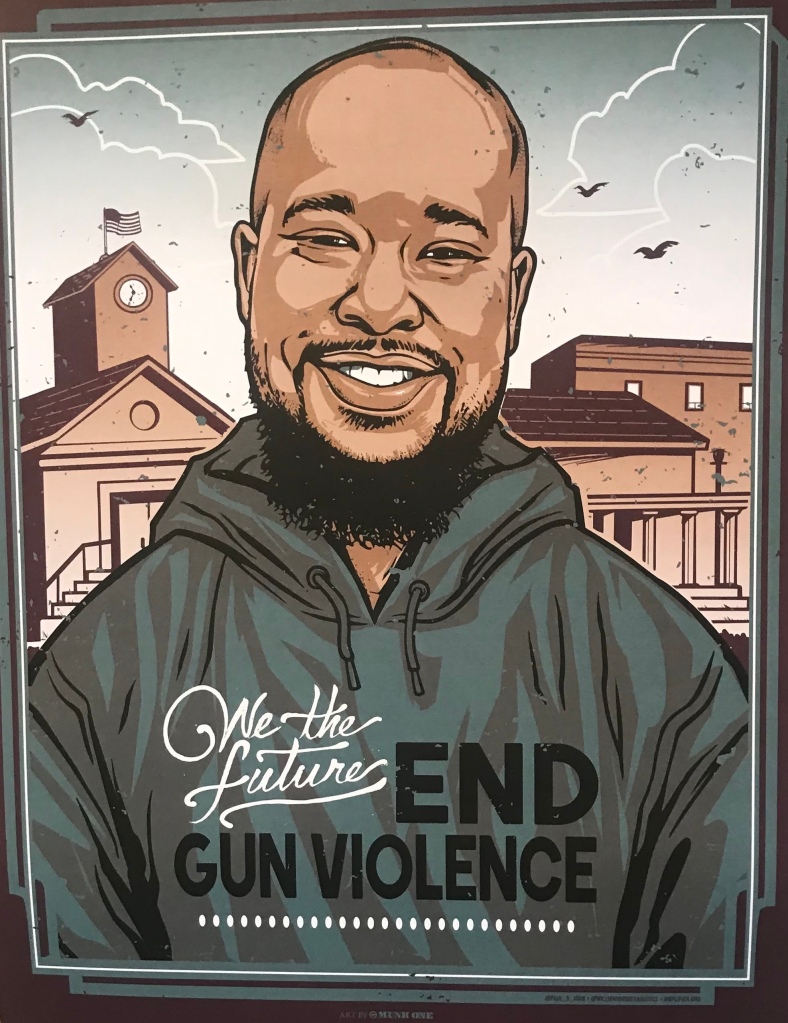
I’ve confiscated guns from high school students, conducted risk of harm danger-to-others 5150 evaluations, and sent texts to my own family, “If I don’t make it home tonight, just know I love you.” For example, when a student (16) posted on Snapchat with a rifle, another student took a screen shot and shared it; The principal called me and said, “I really don’t know what to do, how soon can you get here?”
We met with student and conducted risk evaluation, (similar to suicide risk assessment), spoke with his family, collected the weapon, and made sure there were no other firearms accessible to children in the house.
I’ve co-led trainings on de-escalation with law enforcement, led trauma-informed practices trainings and professional development for educators, child welfare social workers and interns, and behavioral health professionals.
At each training, we ask ourselves, “what more can we be doing to prevent death by gun violence? What more can I do to prevent another gun-violence-at-school tragedy?
Too often we, mental health professionals, tend not to serve or under serve difficult clients with what’s deemed to be volitional behavior. In schools, initial decisions about whether or not behavior will be addressed as a discipline matter (volitional) vs. a mental health a concern, is made by school administrators. Many educational leaders, however, report that they don’t have the level of training needed to evaluate students with potentially dangerous behaviors.
Additionally, even after students are identified as in need of behavioral health support, school counselors and support staff must engage with students and families to obtain informed consent to participate in services. Counselors are less likely to pursue consent for students who say, “I’m not interested in therapy,” even when their behavior demonstrates a need.
Some parents and guardians are reluctant or outright opposed to “mental health” services for their children. Equity and shared vision guides our work and we must acknowledge that many parents, especially parents of color, had negative experiences when they were in school; it’s important to understand the reasons for their caution and hesitations when it comes to mental health services.
Counseling support is often centered around a student’s school day, social emotional learning, and academic progress. Many school personnel meet and communicate with parents and guardians, but few professionals are trained to improve family relationships and dynamics, a key factor in youth mental health. After a tragic loss in mass shootings by school-age youth, bullying and exclusion is often cited as a reason for violence. It’s difficult to question if family dysfunction played a role in violence that occurred, especially if family members were also victims of gun violence. Sadly, this was the case in mass shooting at Robb Elementary School yesterday in Uvalde, Texas (21 killed) and at Sandy Hook Elementary School (26 killed).
School-based Mental Health Programs: Some innovative programs are making inroads engaging families and extended support networks to provide multi-generational support. Even with recent successes and improvements in mental health and school-based mental health programs, we are serving 1 in 5 students identified as needing support services.
Beyond Co-location: Post pandemic, school personnel and partnership agencies have had success reaching out tenaciously to build trust with students and families.
School social workers offer multi-faceted solutions include 5-component “packages of support” that combine professional services, youth enrichment positive activities, and three other people or programs on each child’s team, based on self-determination and each child’s unique needs. Evaluation and referral, care coordination (case management), helps to link students with specialized services, physicians, and child psychiatrists.
Johns Hopkins, UC Berkeley, and The California Student Mental Health Policy Workgroup at CDE have put forward excellent policy recommendations.