First painting, w Julianna Poldi. Learned prep, layering and removing (less is more).
First painting, w Julianna Poldi. Learned prep, layering and removing (less is more).
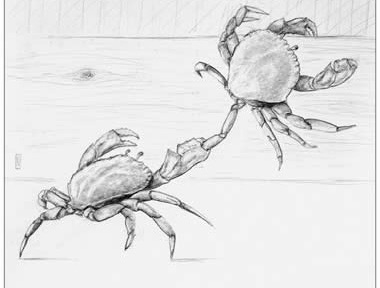
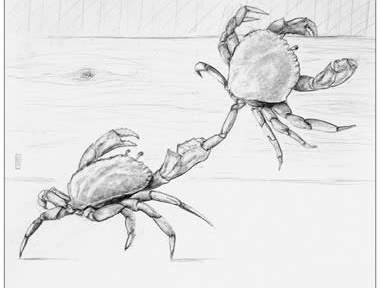
Crabs in a bucket: Marvin (Diné / Navajo) reflected on “Crabs in a Bucket.” An elder in Seattle shared commonly told admonishment that crabs pull each other down, if one tries to climb out of a pot or bucket, other crabs pull it back down. The lesson, be cautious of who is around you.
In nature, however, Crabs actually cooperate, climb on each other, help each other, live in community in order to survive. Their nature is cooperation. The bucket, the elder said, is a Western construct. The bucket is Western society, materialism, individuality. When pulled away from their natural environment, of course crabs behave differently.
A beautiful Native-American re-interpretation of a story commonly told to children; don’t trust or be pulled down by those around you. This stands is stark contrast to Crabs’ true nature, to lift each other up.
Adam Grant (Wharton) added, “We assume this is how crabs behave in a bucket bc this is what we’ve been told. Researchers showed, however, they don’t actually pull each other down. ….Test the hypothesis.”
Native wisdom.
Did you catch this episode of Hidden Brain©️ w Greg Walton @ Stanford? The neurobiology of self-fulfilling prophecies: anticipating negative events contributes to negative events taking place. Walton describes white water rafting w father as a kid; jumped out before rapids, which of course led to capsize.
Also available here;
2nd episode down
Countries where ibogaine treatment centers exist and may offer professional training:
Regarding legal practice of therapist-assisted ibogaine micro-dosing:
Nolan Williams, MD from
Stanford University,researcher w amazing results w vets.
Before pursuing this path, I recommend consulting with a healthcare attorney familiar with international health and mental health policies involving use of pharmaceuticals and plant medicines.
Since regulations around psychedelics are evolving rapidly, verify current legal status in any location you’re considering for practice.
I appreciate your specific questions about ibogaine and psychedelic-assisted therapy. Let me address what I can based on my knowledge cutoff from October 2024.
In the United States, ibogaine is a Schedule I controlled substance, making it illegal to purchase, possess, or distribute. The closest options where ibogaine treatment is available (but not for take-home use) would be:
2. Costa Rica
These locations typically offer on-site treatment only, not take-home quantities, as medical supervision is critical due to ibogaine’s cardiac risks.
There are no formal, accredited training programs specifically for ibogaine microdosing therapy in New Zealand that I’m aware of as of my last update. While ibogaine is a prescription medication in New Zealand, its use is primarily for addiction treatment at specialized clinics, not in standard therapeutic settings.
For broader psychedelic therapy training (not specific to ibogaine), you might explore:
Besides ketamine, common substances being researched or used in some contexts include:
Current legal therapeutic use in the US:
International locations with more established use:
Emerging regions with potentially lower costs:
Average costs:
Ibogaine treatment typically costs $5,000-12,000 USD for a full treatment program at clinics.
This is generally more expensive than ketamine therapy ($400-800/session in the US) but comparable to comprehensive psilocybin retreats ($3,000-7,000).
The field is evolving rapidly, so some information may have changed since my knowledge cutoff.
Claude AI
It’s important to note that all psychedelic-assisted therapies require careful screening, medical supervision, integration therapy, and should be considered within a comprehensive treatment approach tailored to the individual’s specific conditions and history.
🤖- thx Claude.
In Ghana specifically:
Neighboring West African countries:
Countries with more progressive approaches:
Asia generally has stricter drug policies with limited exceptions:
The landscape is evolving rapidly, with clinical trials and research initiatives expanding globally. Several countries are currently reviewing evidence for potential medical applications of various psychedelics, with regulatory changes possible in coming years.
🤖 Claude – u 🪨
When behaviors produces the opposite of the intended result.
Below are examples of well-intentioned behaviors that often backfire socially, along with therapeutic approaches to address them.
Excessive Reassurance-Seeking
Intention: To feel secure and validated in relationships
How it backfires: Creates relationship fatigue, pushes others away, and paradoxically increases anxiety
Therapeutic approach: A therapist might help the client identify underlying insecurities and gradually reduce reassurance-seeking behaviors. “Cognitive restructuring” from CBT could address black and white thinking and over generalization; two thinking patterns that contribute to these behaviors.
Intention: To be useful, needed, and to demonstrate care
How it backfires: Creates dependency, resentment, boundary issues, and burnout
Therapeutic approach: Therapists might explore the client’s core beliefs about self-worth, help them develop identity beyond caregiving, and practice setting healthy boundaries. They might explore family-of-origin patterns that established caregiving as a primary mode of connection.
Intention: To maintain harmony and prevent rejection
How it backfires: Leads to unresolved issues, resentment, disconnection, and eventually larger conflicts
Therapeutic approach: A therapist would help to increase awareness of flight response; and raise the threshold for when the urge to avoid conflict kicks in.
If a client has the ego strength and openness to practicing new ways of being, some therapists use role-playing to practice healthy confrontation, focusing on internal sensations, spirit, and emotions vs. only discussing “what to do.”
Intention: To earn approval and avoid criticism
How it backfires: Creates distance through impossible standards, reduces authenticity, and leads to burnout
Therapeutic approach: Therapy might focus on self-compassion practices, examining the origins of perfectionistic standards, and gradual exposure to “good enough” performance while tolerating discomfort.
Too much Self-Disclosure too soon:
Intention: To create closeness and intimacy
How it backfires: Overwhelms others, creates inappropriate relationship pacing, and can trigger avoidance
Therapeutic approach: Therapists might help the client understand appropriate intimacy pacing, recognize social cues, and develop a wider repertoire of connection strategies beyond emotional disclosure.
Intention: To be liked and accepted
How it backfires: Leads to inauthenticity, unsustainable commitments, and resentment
Therapeutic approach: Therapy would explore fear of rejection, develop identity beyond others’ approval, and use incremental exercises to practice saying “no” and expressing authentic preferences.
Intention: To be understood and prevent misinterpretation
How it backfires: Comes across as defensive, creates doubt in others, and often reinforces negative impressions
Therapeutic approach: A therapist might help identify approval-seeking triggers, practice concise communication, and develop tolerance for being occasionally misunderstood.
Lying or Stretching the Truth:
Intention: To impress others, gain acceptance, or protect self-esteem
How it backfires: Damages trust, creates distance when discovered, and reinforces feelings of inadequacy
Therapeutic approach: A therapist might:
– Explore the underlying feelings of inadequacy or fear of rejection driving the behavior
– Help identify situations that trigger embellishment or lying
– Examine early experiences where the client may have learned that their authentic self wasn’t “enough”
– Work on developing self-acceptance and recognizing inherent worth
– Practice vulnerability in safe settings, starting with small truths
– Role-play managing the discomfort of being perceived as “ordinary”
– Gradually build confidence in authentic self-presentation
– Create a hierarchy of truth-telling challenges, from low to high risk
– Acknowledge and process shame that may arise from both the behavior and addressing it
The therapeutic relationship would offer a space where complete honesty is encouraged without judgment, helping establish a new pattern of authentic connection that can extend to other relationships.
In addressing these other patterns described above; therapists typically employ several key approaches:
The therapeutic relationship itself often becomes a space for honest self reflection; a starting place for shifting patterns in real-time. Through self determination, a clients in therapy decide which behaviors they wish to generalize to other settings.
